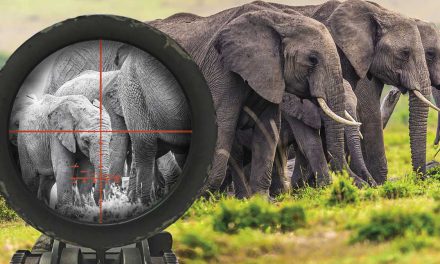
Zimbabwe’s Constitution clearly stipulates the right to clean, safe, potable water but poor governance makes this a pipe dream for most citizens

Most major cities in African countries are currently characterised by significantly large population increases. This is attributed partly to rural-urban migration as urban centres are perceived as having better standards of living and a myriad of opportunities. Population figures are expected to continue to climb due to both natural growth within cities and as people from elsewhere seek better lives. The rural-urban movement has also been attributed to changes in climate; in some instances, extreme weather conditions such as droughts and floods have impacted food production and this has forced rural populations to seek alternative forms of livelihood.
The problem lies in that African cities have not developed their infrastructure beyond what was left by colonial governments. In some instances, the infrastructure is derelict, worsened by industry that is either stagnant or not growing in proportion to the burgeoning population. Other cities are in countries that face political upheavals of various kinds that adversely affect the economy, let alone developmental work. A combination of factors such as poor or a lack of governance, a weak economy and a lack of development have rendered most cities ill-equipped for the rise in population and the requisite infrastructural rural demands to cater for the increase. This is in spite of the bodies of fundamental principles that should ideally be used to govern states.
Using Zimbabwe as a typical example, the Constitution of Zimbabwe Amendment Act 20 of 2013 in its Declaration of Rights clearly stipulates the right to water among other rights, and section 77 distinctly outlines the rights to water for all citizens by stating that: “Every person has a right to (a) safe, clean and potable water and the state must take reasonable legislative and other measures, within the limits of the resources available to it, to achieve the progressive realisation of this right.”
In line with this, the state has a responsibility to ensure the right to water is fulfilled, promoted and protected. There are Acts in place that include, but are not limited to, the Public Health Act, the Water Act of 1998 and the Zimbabwe National Water Authority (ZINWA) Act of 1998 that address the significance of the right to water. The Public Health Act has sections that stipulate the provision and maintenance of sufficient sources of pure water for drinking and other domestic uses by all local authorities. The ZINWA Act focuses on ensuring exploitation, conservation and management of water resources in Zimbabwe. Its objectives include ensuring equal access, allocating water efficiently, distributing and providing enough water at reasonable costs, to cite a few.
The right to water, among other rights, is undoubtedly central as the essence of life hinges upon water. Water is intricately linked to other rights such as the right to health or the right to a safe and clean environment, and all these aspects are crucial elements that allow people to live in dignity. Against this backdrop of rights, according to UNICEF Zimbabwe, the country experienced a cholera outbreak in 2008-2009 in which 100,000 people were affected and 4,000 died, despite such explicit provisions in the Constitution and in the Acts. UNICEF points out that 25% of households in the country do not have any type of toilet facility, according to the 2012 National Population Census data. The Multiple Indicator Cluster Survey, carried out in 2014, showed that open defecation, mostly in rural areas, was at 31.7%, but such practices also extended into urban centres due to dysfunctional service-provision structures.
Exactly 10 years later, Zimbabwe is faced yet again with another cholera outbreak, and this raises genuine concerns. Cholera is caused by ingesting bacteria found in contaminated food or water. Zimbabweans find themselves tangled up in water constraints to the extent that cities and rural areas face cholera outbreaks in spite of the constitutional stipulations and various Acts. Instead of improving from its 2008 plight, the country is entangled in a reoccurrence within a space of nine to 10 years. Past experiences have not led to preparedness or an understanding of the consequences of failing to meet the right to water and this has manifested in a disease outbreak that could have been easily avoided.
Many areas within the urban centres have gone without piped water for years and are filled with raw, untreated sewage along the streets, which begs the question on how the sanitation facilities have been running. On one hand, water-access issues in the rural areas are ignored and concealed from the public while, on the other hand, the cities have defunct infrastructure.

Sunset from a boat over the Zambezi, Victoria Falls, Zambia / Zimbabwe border
According to a 2013 UNICEF Zimbabwe report, over four million people in Zimbabwe, about a third of the population, lack safe drinking water. This is tied directly to ReliefWeb 2018 statistics, which show that in the period between January to May 2018, 177 cholera cases were reported as well as 17 deaths. By September 2018, 1,901 cases had been reported, with 58 confirmed cases, 1,843 still under investigation and 24 deaths. Zimbabwe has reported cholera cases for the past three years, albeit on a lower scale. A correlation exists in that cholera cases were reported in areas hardest hit with water shortages such as Budiriro and Glen View in Harare, but extending to areas such as Buhera, Chitungwiza, Shamva, Gokwe North, Makoni and Masvingo districts. The number of people estimated to be at risk is 200,000 as cholera is endemic to the country.
A number of contributory factors, such as the unpaid water accounts in urban areas that were written off in politically motivated campaign initiatives in 2013, played a part in infrastructural collapse. Most residents also queried paying for services they were not getting. On another level, the city authorities disconnected water services for anyone who was unable to pay, forcing people to use unsafe water options. The water charges have also proved untenable for most residents, who in some areas face perennial water shortages. The few payments that are made have not been channelled back into water provision but instead diverted to other uses in violation of city-budget guidelines. Most local municipalities are, therefore, in dire straits and cannot meet their obligations to the general populace. This state of affairs has contributed to local authorities’ failure to purchase the required chemicals used in treating water, a situation perpetuated by the state of the economy and ultimately resulting in less potable water.
Human Rights Watch (HRW) in Zimbabwe rightly cites corruption and government mismanagement (at all levels – local, provincial and national) as some of the major contributory factors to the water crisis and consequently to cholera outbreaks. A HRW survey found that residents had resorted to drinking water from unprotected shallow wells and defecating in open spaces, conditions conducive to disease outbreaks and which are in direct violation of the rights to safe water. An unsettling account in the HRW report describes a household of 21 people with one toilet that does not flush, leaving them to use buckets to flush the toilet or resorting to using the bush. Residents had also resorted to using boreholes as these were perceived to be safer alternative sources of water.
Zimbabwe has provisions to control borehole drilling and drillers, which ordinarily would not be a problem. These, however, expose the failure of the state and its instruments to provide basic water services, thereby forcing residents to seek alternatives. According to HRW, 200 boreholes were drilled by international agencies in the aftermath of the first cholera outbreak, but these do not take into account the numerous boreholes residents have drilled for themselves. It is unsurprising, therefore, that tests conducted by Harare Water revealed that the water from a third of these boreholes was contaminated, given that the sewerage system as a whole is dilapidated and seepage from broken pipes easily compromises borehole water.
A lack of investment in water and sanitation systems in Zimbabwe has led to the water-related crises the country faces. The response of the ruling party and opposition in the recent cholera outbreak has been discouraging, hurling blame at each other without actually addressing the situation. The lack of water extends to health facilities within the country, posing an additional threat to an already precarious situation. The Zimbabwe National Water Authority (ZINWA), which is meant to supply and manage domestic water in urban areas, has failed to properly carry out this mandate. The water from the taps is dirty, discoloured, and has contributed to the outbreaks of disease and stomach problems. In as much as the legislation and policies on WASH (water and sanitation hygiene) are unquestionable, they are not fully implemented amidst an ailing system of water provision. This has left citizens vulnerable, regardless of the commendable legal stipulations existing within the country.

PRUE MUTUMI has a PhD from the University of the Witwatersrand School of Geography, Archaeology and Environmental Studies. She also has a MA Heritage degree from Wits and a BSc in tourism and hospitality management from the University of Zimbabwe. She has served as a board member of the Johannesburg Heritage Foundation